
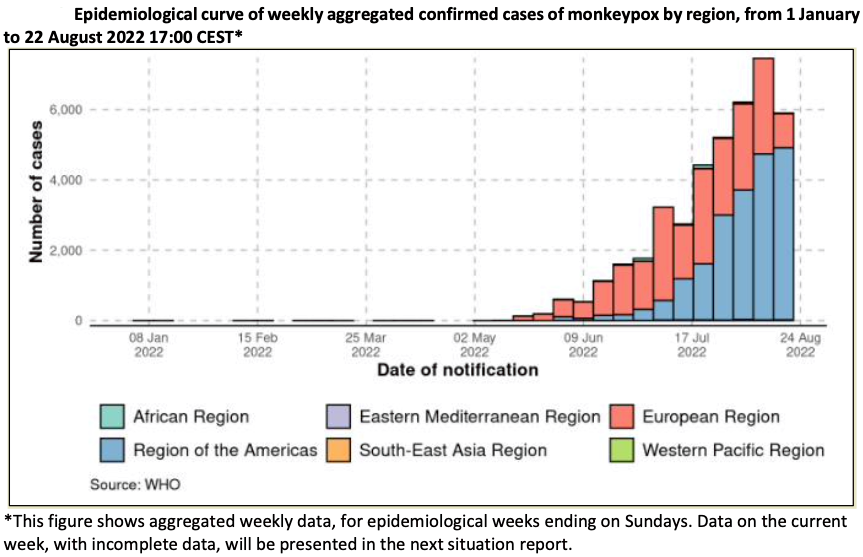
Geneva: During the week of August 15 to 21, 2022, the number of monkeypox cases reported in the Region of the Americas shows a continuing steep rise, confirming trends seen over the last several weeks.
From January 1, 2022, through August 22, 2022, in all 41 664 laboratory-confirmed cases of monkeypox and 12 deaths were reported to WHO from 96 countries, stated the ‘External Situation Report 4’ on the multi-country outbreak of monkeypox, which was revised today to correct the number of cases reported in week 32 (August 8-14, 2022) from 5213 cases to 7477 cases.

Since the last edition of this report published on August 10, 2022, in all 13,859 new cases (50% rise) and 1 new death were reported; and 7 new countries reported cases. As of August 22, the ten countries that reported the highest cumulative number of cases globally were the United States of America (n = 14 049), Spain (n = 6119), Brazil (n = 3450), Germany (n = 3295), The United Kingdom (n = 3225), France (n = 2889), Canada (n = 1168), Netherlands (n = 1090), Peru (n = 937), and Portugal (n = 810). Together, these countries account for 88.9% of the cases reported globally.
In the past seven days, two countries, Iran and Indonesia, reported their first case, while 23 countries reported a rise in the weekly number of cases, with the highest rise reported in the United States of America. There are 16 countries that have not reported new cases for over 21 days, the maximum incubation period of the disease.
The outbreak continues to affect young people of the male gender, with 98.2% (20 138/20 500) of cases with available data on the gender being males with a median age of 36 years (Interquartile range: 30-43 years). Fewer than 1% (140/23 626) of cases with age data available are aged 0-17 years. This proportion differs between countries, with those in West and Central Africa reporting a greater proportion of cases among young age groups: 38.7% (65/168) of cases for whom age was available were among the age group 0-17, out of which 12.5% (21/168) were aged 0-4.
Among cases with sexual orientation reported, 95.8% (9484/9899) identified as men who have sex with men. Of all reported types of transmission, a sexual encounter was reported most commonly, with 5954 of 7250 (82.1%) of all reported transmission events. The majority of cases were likely exposed in a party setting with sexual contacts, with 2204 of 3639 (60.6%) of all likely exposure categories. Among cases with known HIV status, 45% (4501/10 036) are HIV positive.
Globally, after four consecutive weeks of increase, the number of monkeypox cases reported declined by 21% overall during the same week (n=5907 cases) as compared to the previous week (n=7477 cases). This decrease may reflect early signs of a declining case count in the European region, which would need to be subsequently confirmed.
On August 8, WHO convened a meeting of two of its collaborating centres for orthopoxviruses and other experts in poxvirology and viral evolution to consider the naming of monkeypox virus (MPXV) variants. Henceforth, the Congo Basin or Central African clade will be referred to as Clade I; the West African clade will be referred to as Clade II, with subclades IIa and IIb, the latter referring to the variant that is predominant in the multi-country outbreak.
WHO also updated the interim guidance on vaccines and immunization for monkeypox. Updates include a clearer emphasis on the groups at risk of monkeypox for consideration for preventive vaccination and updated terminology for pre- and post-exposure vaccination. To reduce confusion with the terms used in the management of HIV, the changes include using primary preventive (pre-exposure) vaccination (PPV) rather than pre-exposure prophylaxis (PrEP), and post-exposure vaccination (PEPV) rather than post-exposure prophylaxis (PEP).
– global bihari bureau


